


Broken bones and fractures
General principles

Bone fractures are usually caused by the action of mechanical force on a bone that splits it in two or more fragments.
The fragments can remain inside the tissue without piercing the skin, thus talking about closed fractures, or piercing the tissues and skin and bursting out, when talking about open fractures. In any case, open fractures are riskier due to the the high risk of infection. When the bone is infected, the healing process is time-consuming and painstaking, so every effort should be made to minimize the risk of infection.
Sharp bone fragments damage adjacent tissues and cause severe pain, and can interrupt blood vessels, causing bleeding, the severity of which depends on the size of the blood vessel.
The basic principle of fracture management is immobilization. Immobilization (placing the bone in a fixed position) reduces the pain and damage to the adjacent soft tissues. Relieving of pain reduces the possibility of shock. Adjacent joints on both sides of the fracture need to be immobilized.
Signs that indicate a possible closed fracture are:
- information about the fall, impact of a heavy object or the effect of another, strong force on the limbs or body parts
- the injured, or those close to him, heard the sound of a bone cracking
- swelling and deformity are evident: the broken part of the body is in an unnatural position
- inability or aggravated, painful movement of the broken limb.
Principles of Fracture Management

In the case of a complicated fracture or fracture of the pelvis, upper leg, spine and head bones, medical advice should be sought immediately by radio.
When there is no risk of further injury, the fractured casualty, if bleeding, should not be moved until the bleeding has stopped and the fracture has been immobilized.
Take these actions while waiting for medical help:
- Stop any bleeding. Put pressure to the wound with a sterile gauze, a clean cloth or a clean piece of clothing.
- Immobilize the injured area. Do not attempt to realign or push back in a bone that is sticking out. If you have been trained in how to splint and professional help is not available promptly, apply a splint to the area above and below the fracture sites. Padding the splints can help lessen the discomfort.
- Apply ice packs to reduce swelling and help relieve pain. Do not apply ice directly to the skin. Wrap the ice in a piece of cloth.
- Treat for shock. If the injured person feels faint or is breathing in short, rapid breaths, lay the him down with the head slightly lower than the trunk and, if possible, elevate the legs.
Bleeding in fractures
Bleeding from an open fracture should be stopped in the usual way (using sterile gauze and pressure on the wound, compression bandage, blood clamps). Blood does not come from the broken bone but from the surrounding area: broken tissue and blood vessels. A broken limb should always be lifted (although it is painful) as this reduces blood flow and bleeding intensity. The bleeding should be stopped because people do not die from broken bones, but because of exsanguination. Rest reduces further bleeding, prevents further injury and pain.
When the bleeding has been stopped, the wound should be treated. The wound area is cleaned and disinfected with warm water and soap and 1% Cetavlon solution. Water, soap and disinfectant must not enter the wound. The wound must be covered with sterile gauze during this time. If there are foreign bodies in the wound (pieces of clothing, stones, wood, metal, etc.), they should be carefully removed with sterile tweezers. The bandage that stopped the bleeding should not be immediately removed even though it has been soaked in blood, because in that case the bleeding will recur. Such a wound should not be sutured.
A doctor via radio should be consulted about further procedure.
Pain management

Severe pain should be suppressed by administering 1 ampoule (10 mg) of morphine hydrochloride to the muscle. For fractures of smaller bones, milder painkillers (analgesics) may be given in tablets or in injections.
When administering morphine, the advice of a physician via radio should be sought before repeating the dose. In order to avoid intense pain, the broken part must be handled with care.
Immobilization

There are different types of splints for immobilization. Splints, regardless of the type, are placed over the bandage, which stops the bleeding and takes care of the wound. The splint must be long enough to cover both adjacent joints of the broken bone.
Pneumatic splints are used mainly for the injured who are transported on board or to the hospital. When placed, they should not remain on the broken part for more than 4 hours as they interfere with circulation, other immobilizing agents may be used thereafter. The broken part of the body is immobilized in its natural (physiological) position, which means in the most comfortable position possible when the muscles are relaxed. For example, a broken forearm will not be immobilized with a stretched arm but bent at the elbow. However, if there is a fracture in the elbow and the arm cannot bend, the arm will be immobilized in a stretched position.
A broken arm or leg should be carefully stretched unless we are dealing with a complicated fracture. In this case, the foot or the palm is grasped and the limb is stretched slightly, then slowly placed in the immobilization position. It must not be done violently or with great force.
When there is no dedicated immobilizer, the fracture can be immobilized with a wooden strip/board that has previously been wrapped with a towel, gauze or cloth.
Spinal injuries should be immobilized on a wide plank or door.
Instead of a triangular bandage, the front of the jacket can be folded and secured with a safety pin to immobilize a broken forearm, and to immobilize other smaller parts of the body, a square cloth folded to a triangle can be used.
Circulation check

The presence of circulation in a broken limb should be checked by checking the pulse and/or pressing the nails. If circulation is normal, the nails turn pale when pressed and pink when the pressure subsides.
Warning signs are:
- absence of pulse
- blue or pale fingertips
- cold parts peripherally from the fracture
- loss of sensation and tingling of the peripheral part of the broken limb
Signs of circulatory disorders should be checked frequently. When present, consult a doctor via radio as a matter of urgency to avoid amputation.
In fractures, the possibility of internal bleeding should not be overlooked, and therefore the signs described in internal bleeding should be controlled.
Upper jaw fracture
In facial injuries, airway patency should be taken into account. When there is bleeding with the fracture, it should be stopped. Broken teeth are not instantaneously removed unless there is a risk that they may be swallowed or enter the airways.
Severe blows to the mouth and face may result in a jaw fracture with tooth loss, gum injuries, injuries to the lips, soft cheeks and tongue. External wounds on the cheeks and lips should be taken care of standardly.
In the case of injuries to the inside of the mouth, the injured person must first rinse the mouth with clean water and spit out any severed parts (e.g. teeth). No attempt should be made to remove any parts that still adhere to the remaining tissue. If the injured person is in pain, they should be given painkillers in the muscle. Do not attempt to suture internal sores in the mouth. Serious bleeding should be stopped by pressing.
If the upper or lower jaw is broken or in cases of suspicion of a fracture, the jaw should be immobilized so that the teeth of the upper jaw touch the teeth of the lower jaw.
For oral wounds, antibiotics should be given to prevent infection. To this end, benzylpenicillin with procaine-benzylpenicillin should be administered to the muscle for five days.
Make sure you consult your doctor by radio.
Lower jaw fracture
Lower jaw fracture can cause deformity, tooth loss, bleeding from the gums, swelling and difficulty swallowing.
Injury management: A fractured jaw may cause breathing difficulties. In this case, the jaw and tongue should be pulled forward and held in such a position that the injured person can breathe. The problem is even greater if both sides of the jaw are broken since they can fall backwards together with the tongue and obstruct the airways. In this case, the finger should be placed behind the front teeth of the lower jaw and pulled forward, and the injured person needs to be transported in a sitting position.
When the spasm of the jaw muscles (due to pain) occurs, then the teeth of both jaws are clenched tightly, and this prevents the lower jaw from sliding back. It is painful for the injured, but it is better to stay in this position because it keeps the lower jaw immobilized. The jaw can be immobilized with a bend or two triangular bandages.
If the injured person is unconscious, one should pull the lower teeth forward and place the casualty in a resting position. Due to the risk of suffocation and bleeding, the injured person should not be left unattended. You should definitely seek medical advice via radio. For pain control, analgesics or morphine should be given.
Fractured collarbone and shoulder
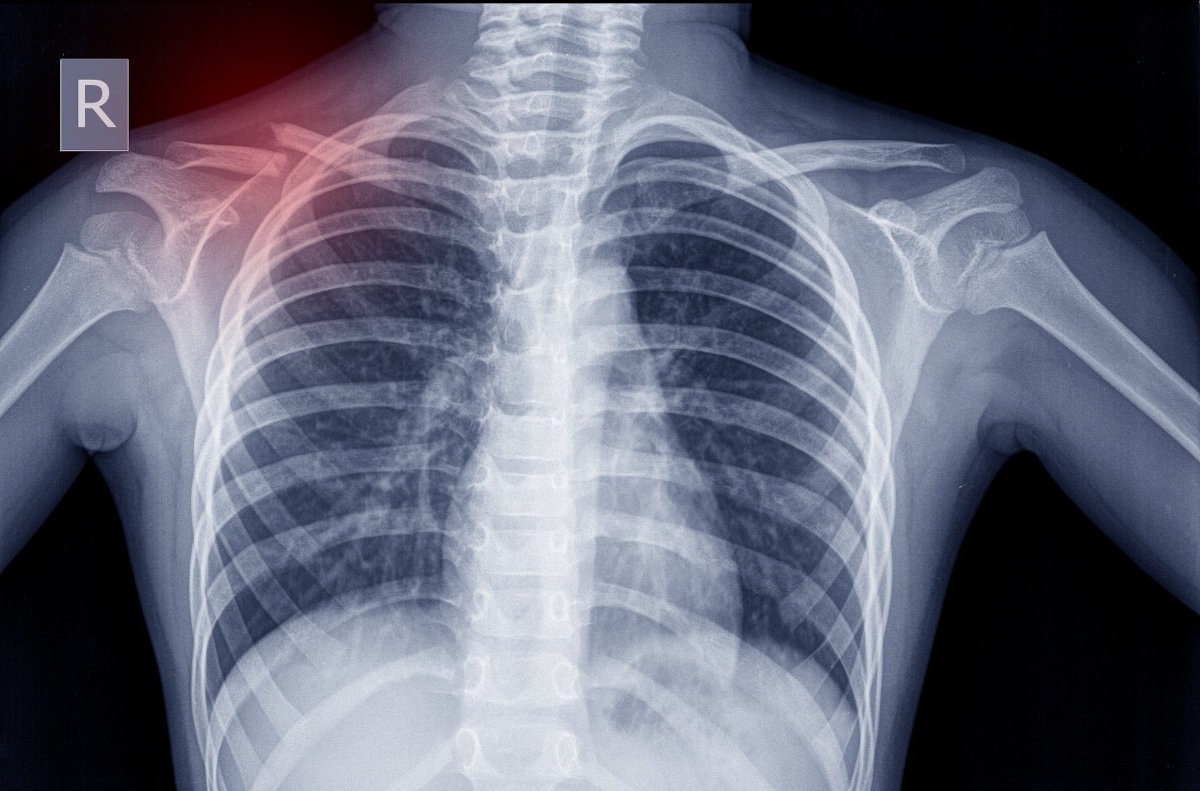
These fractures usually occur when you fall on your shoulder or arm. Direct hit is a rare cause of fracture. If only the collarbone is broken, hold the arm close to the body with the other arm or a sling with the hand raised higher than the elbow.
The arm should be moved as little as possible. An ice pack wrapped in a towel should be applied directly to the broken collarbone. A homemade sling can be formed from a large handkerchief, or towel, or from the triangle bandage.
In some shoulder bones fractures the arm should be immobilized, for which a triangular hem is very suitable. Most fractures of the body of the scapula are treated without surgery. Ice is used for swelling, and pain medications are used for pain control.
Fracture of upper arm, elbow and forearm
In fracture of the upper arm and elbow, the impaired function is expressed in the inability to raise the arms or bend the elbow. Fracture of the upper arm can be complicated by injury to the arteries and nerves that are in the immediate vicinity of the bone.
Procedure: The upper arm and elbow should be immobilized with a pneumatic mould or classic Kramer joint in a flexed elbow position. A broken elbow is difficult to bend due to pain and complications, so the arm must be immobilized in the extended position.
The forearm has two bones: the thumb (radius) and the elbow (ulna). They can be individually or both broken. Usually a fracture is the result of a fall on the arm, only exceptionally due to the direct action of the force.
Procedure: First, carefully stretch the broken bones by grabbing the palm and upper arm of the broken arm, then immobilize. Immobilization can be performed by inflatable splinters, classic Kramer splints or improvised immobilisers.
Pain should be suppressed by the use of analgesics.
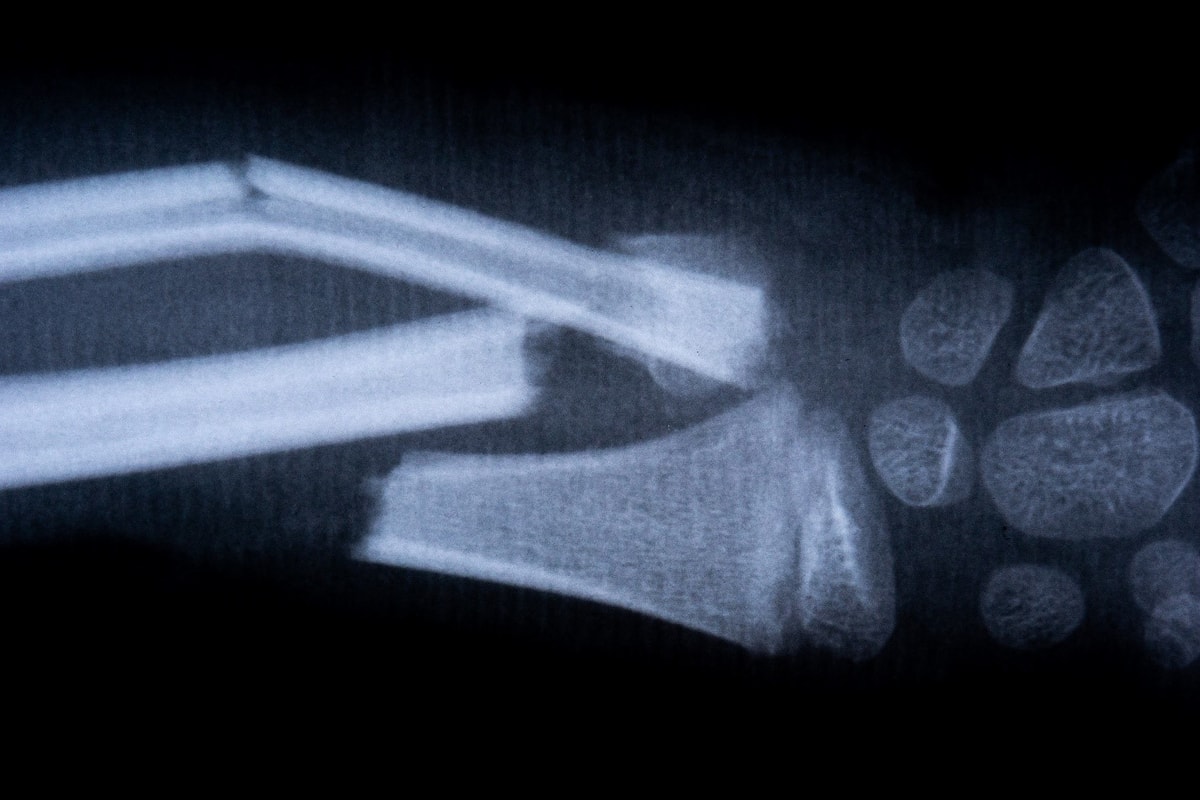
Fractures of wrist, hand bones and fingers

The wrist usually breaks when an individual falls on the outstretched fist.
Fractures of the bones of the fist can be the result of direct impact or bruising. They are accompanied by swelling, pain, unnatural appearance, impaired function, and sometimes an open wound. The fist should be immobilized on a straight splint and a lump of cloth or bandage should be inserted into the fist cavity.
The fractured joint should not be "pulled" but immobilized. If severe pain is present, analgesics should be given. The injured fist should be lifted up to reduce bleeding and swelling. Hand bleeding should be handled in the usual way.
The forearm is attached to the splint with a bandage.
When a finger fractures, only the broken finger should be immobilized, and the rest must be free. Before immobilization, the injured finger should be "pulled out" slightly. It should be immobilized with a wooden stick.
Spine and neck fractures

Fracture of the spine is one of the most serious and dangerous injuries. When there is a suspicion a fracture of the spine occurred, the injured person should lie down on a hard surface and forbidden further moving. Any movement can cause the spinal cord to intersect, which, depending on the seriousness of the injury, causes lifelong limb paralysis and the inability to control stools and urine.
When the injured person cannot lie down on a hard surface by himself or when he is unconscious, the he must be laid down by three people simultaneously and harmoniously. He is mobilized on a rigid base, to which his feet and the body are tied. Wraps of fabric are placed under the neck and back. These procedures must prevent vertical and horizontal movement and reduce the possibility of damage to the spinal cord.
When carrying an injured person, he must be carried by six people. One holds him by the head and stretches it slightly, while two people hold him on each side. He is placed on a blanket and the ends of the blankets are rolled up. The people who are sideways lift the injured person holding the blanket by the curved side edges. They must also work harmoniously in order to prevent additional damage.
Casualties with a spine fracture that can be extremely severe should be given severe analgesics or morphine. For further procedures, be sure to seek medical advice via radio.
Injuries and fractures of the neck occur as a result of a blow to the head, a fall to the head or legs or a direct effect of force on the cervical spine. First aid procedure is similar to spinal injuries considering that the neck is a part of the spine. The injured should lie on his back and his neck should be immobilized with a dedicated Schanz collar. In the absence of a dedicated immobilizer, the neck can be immobilized with several layers of newspapers.
Chest injuries
Injuries and fractures of the ribs are usually caused by falling on sharp and solid objects or action of a strong force (impact) to the chest. They are accompanied by severe pain that is exacerbated by breathing. The lungs can be damaged when the injured person has difficulty breathing and his cough is accompanied by bloody spit. The pulmonary pleura (visceral pleura) can be pierced with sharp rib fragments that can lead to a collapse of the lungs (pneumothorax).
If it is an open wound to the chest, it must be closed immediately, otherwise the air will enter the chest cavity and the lungs will collapse. In such situations, the wound should be closed as soon as possible. The wound is first covered with a layer of wide Vaseline gauze over which aluminum or plastic foil is placed. After that, both layers are firmly fixed with Leukoplast tape.
External bleeding is stopped by putting pressure on the wound.
The injured, if conscious, rests in a semi-sitting position. Due to the possibility of internal bleeding, the pulse and other signs of bleeding must be constantly monitored. The frequency of breathing must also be monitored. The injured with a chest injury, after the wound has been taken care of, is placed in the resting position on the injured side. This will prevent bleeding from starting and bleeding out into the chest. The head can be turned and positioned down (if possible) to help keep the airways open. When blood foam comes out of the mouth or nose, it should be cleaned by using an aspirator or wiping with gauze.
In case of suspected chest injuries, and especially for injuries complicated by pneumothorax, seek medical advice by radio.
Pneumothorax is a very serious injury that requires consulting a doctor via radio and transferring the patient to the hospital by helicopter. When transporting an injured patient with pneumothorax, the helicopter must fly low and avoid making sudden changes in altitude.
Injuries and fractures of the pelvis

The fracture of the pelvis usually occurs after a strong impact, that is, a direct effect of force on the pelvic bones. The injured feels pain in the hips, bottom of the abdomen, groin, lower back or thighs.
When a pelvic bone fracture is suspected, a simple test consisting of careful, gentle, circular pressure on both lateral pelvic bones downwards is applied. This procedure will increase the intensity of pain if the pelvis is broken. Sometimes, when performing this test, the movement of broken pelvic bones can be felt.
If the bladder and the urethra are injured, the urine can penetrate the surrounding tissue. The injured person should not be made to urinate, but if he does, a urine sample should be taken and tested for blood.
Fracture of the pelvic bones can cause severe internal bleeding into the lower abdominal cavity. Therefore, the injured person should regularly be checked for pulse and other signs of internal bleeding.
When you suspect pelvic injuries have occurred, seek medical attention via radio.
The injured person should be carefully lifted and transported, only in the supine position. To transport him, he must be immobilized so that one splint is placed from the armpit to the end of the leg and the other from the inside of the groin to the end of the leg. The splints should be tied and fastened with straps (handkerchiefs, bandages, pieces of cloth, etc.). If we do not have a splint, lay the injured on a sufficiently wide plank and secure him as you would with a fracture of the spine. For pain management, strong painkillers or morphine should be given. Remember to measure the patient's pulse regularly and check for other signs of internal bleeding. If the victim is in shock, follow the instructions for shock treatment.
Fracture of the femur

Injured with a fracture of the femur feels severe pain and cannot move his leg. The broken leg looks shorter and abnormally twisted (rotated). Due to bleeding and pain shock can occur. In this case, you should seek medical advice via radio. Also, even in the fracture of the neck of the patella there is usually a leg deflection and an outward rotation.
If you suspect a closed fracture had occurred, the broken leg should be carefully immobilized. Splints should be wrapped with soft material, placed on the outside and inside of the leg, and tied together with straps.
If both legs are broken then place fabric inserts between the two legs, the coated splints with a thicker layer of fabric on the sides of the legs (from the armpit to the feet) and fasten it all with ties.
Sometimes a fracture of the femur can cause serious bleeding that can be life-threatening.
Fractures of the lower leg, ankle and foot

The lower leg has two bones - the thicker, inner one (tibia) and the thinner, outer one (fibula). Fractures of these bones usually occur after a severe blow or fall.
With a closed fracture of the lower leg, there are: swelling, deformity, impaired function and pain.
Procedure: The shin should first be carefully pulled out by pulling gently by the sole. Classical or inflatable splints may be used for immobilization. For complicated (open) fractures, inflated splints have the advantage of helping to stop bleeding. When using a classic splint, it should be well wrapped with a soft material, one should be placed on the back and the other two on each side of the broken lower leg. The joints that tighten the knee and the ankle joint extending from the hip to below the feet should be interconnected.
A fracture of the ankle and foot usually occurs after a fall, "twist" of the leg or impact. Pain, swelling and impaired function are expressed.
Procedure: If available, it is a good idea to apply an inflatable splint to the lower leg for immobilization. Otherwise, the ankle should be protected from blistering before putting on classic splinters. The splints should be placed so that they go over the foot and on each side of the foot to the middle of the ankle. When there are no classic splits, improvisation can be done with a blanket or pillow.